
VBAC Options & Birth Statistics: Hernando County Edition | Spring Hill Home Birth Midwife
Hello families! This blog was originally going to be a “VBAC (vaginal birth after cesarean) options in Hernando County”, as I have been noticing a lot of women in the local breastfeeding facebook group asking about VBAC-friendly providers. The more I started digging into Hernando’s cesarean rates vs successful VBAC, the deeper into the rabbit hole I fell. The numbers are alarming and unpromising, to say the least. We’ll get into those in a minute. But first we’ll talk about why VBAC is an appropriate option, who is a candidate for VBAC and what all of the professional organizations have to say about cesareans and VBAC.



Breaking down safety, research & statistics
Want to know what ACOG & AAFP & WHO have to say about cesareans and VBAC? You can check out their statements by directly following the links included below!
The World Health Organization (WHO) recommends a healthy cesarean rate to be 10-15% of all deliveries. They’ve discovered that when rate of cesarean delivery is around 10%, the occurrence of maternal and neonatal deaths decrease. But if the number of c-sections increase above 10%, mortality rates do not improve.
The American Congress of Obstetrics and Gynecology (ACOG) practice bulletin #54 issued in 2004, supports a woman's right to choose VBAC, but states that patients attempting VBAC should have "physicians immediately available to provide emergency care". This position was first stated in a practice bulletin issued by ACOG in 1999. This has been interpreted by hospitals to mean that there must be a constant presence of a surgical team, including an obstetrician and anesthesiologist on premises, the entire time a woman is in labor. ACOG updated their practice bulletin in 2010, lessening restrictions on vaginal birth after cesarean and trial of labor after cesarean (#115). Where they admitted that the cesarean section rate is “undeniably high and concerning” and that most women should be counseled on the risks and benefits of TOLAC & VBAC. But they still recommend a TOLAC be attempted *only* in a facility with a physician and anesthesia, in the event of a uterine rupture.
The American Academy of Family Physicians (AAFP) presented a review of information on VBAC in March 2005 and issued recommendations that continued to support VBAC. Their recommendation included "TOLAC should not be restricted to facilities with available surgical teams present throughout labor since there is no evidence that these additional resources result in improved outcomes." This is NOT an endorsement of out-of-hospital VBAC! They simply found that there was no merit to the ACOG recommendation, that the continuous presence of an obstetrician and anesthesiologist improved outcomes in any way!
AAFP *also* stated that VBAC is “safe and appropriate for most women with history of 1 or 2 prior cesarean deliveries.” And goes on to also say that even women with an unknown incision type or more than 2 cesareans should also be counseled on the risks and benefits of VBAC and that having more than 2 prior c-sections does not disqualify them as a VBAC candidate.
(http://www.who.int/mediacentre/news/releases/2015/caesarean-sections/en/)
(http://www.acog.org/About-ACOG/News-Room/News-Releases/2010/Ob-Gyns-Issue-Less-Restrictive-VBAC-Guidelines)
(http://www.aafp.org/dam/AAFP/documents/patient_care/clinical_recommendations/AAFP%20PVBAC%20guideline.pdf )
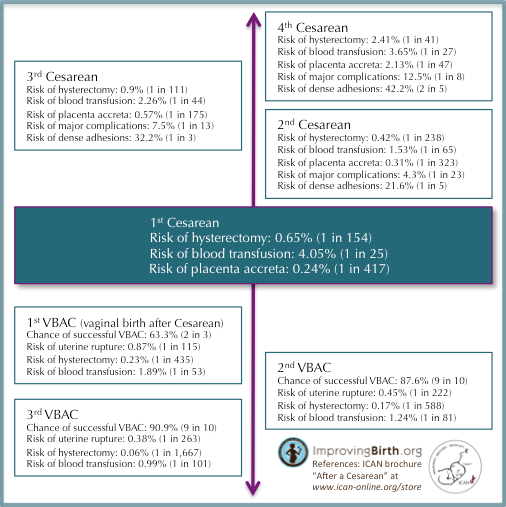
Actual risks
Maternal morbidity: significantly lower risk of maternal death if labor begins spontaneously, regardless of mode of delivery (4:100,000 TOLAC vs 13:100,000 repeat cesarean without spontaneous labor)
Uterine rupture in *primary* VBAC: 0.3-0.9%
Currently ACOG (and most OB-based providers) recommend 18 months or more between deliveries to lower this risk, your body needs a lot of time to heal after a major surgery such as cesarean delivery (HOWEVER, this does not mean that you should not be encouraged to TOLAC, nor does it disqualify you as a good candidate for a VBAC!)
Women planning repeat cesarean deliveries *will* incur increasing risks of uterine rupture, abnormal placentation, hysterectomy & other potential surgical complications
One study showed repeat cesarean deliveries performed before 39wga, is associated with neonatal respiratory distress, NICU admission, need for ventilation and prolonged hospitalization for mom & baby
The reality of cesarean in Hernando County
All of the following information was retrieved from www.floridacharts.com, which is available to the public.
Among mothers residing in Hernando County FL there were 1600 live births in 2015
610 of those births were via cesarean (38%)
Of those cesareans, 385 (63%) were primary and 225 (36%) were repeat
And only 9 women had a successful VBAC. 1 VBAC was a planned home birth with a licensed midwife
Only 8 women successfully VBACed in the hospital…
What’s wrong with this picture?
That’s a .5% (yup - half of a percent!) chance of achieving a VBAC, in Hernando County hospitals.
Do those seem like good stats to you? Remember WHO’s recommendation? How about what ACOG & AAFP said? It is very clear, that the women who deliver via cesarean, are not being properly counseled on TOLAC/VBAC nor are they being given an actual opportunity to attempt them. According to this number, it seems as though the women who were able to achieve a VBAC, must’ve walked in pushing their babies out… I’d love to hear their birth stories either way!
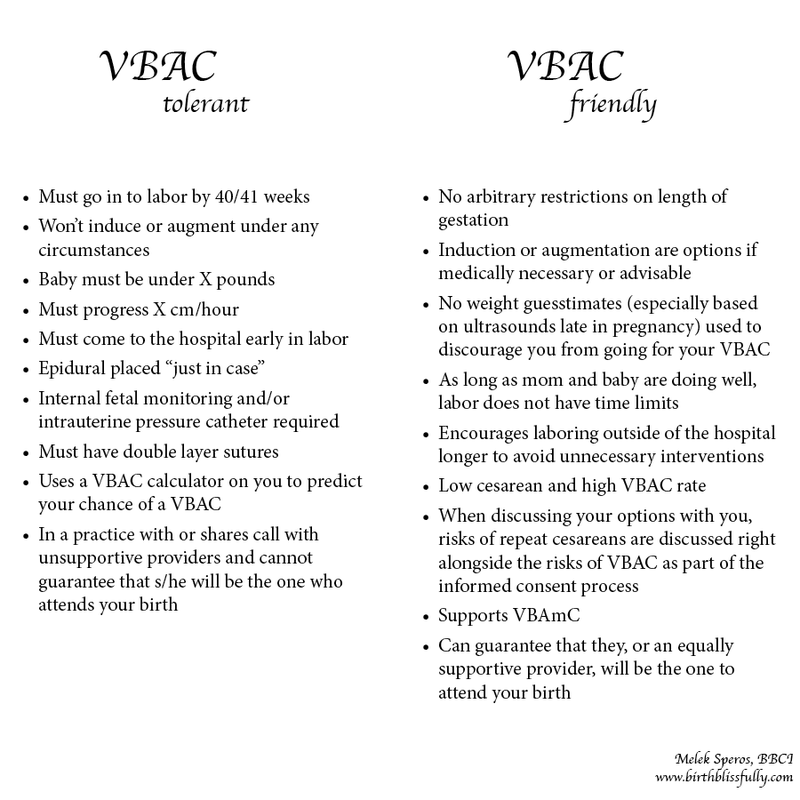
How to recognize red-flags with your provider
(Yes, I’m referring to out-of-hospital based midwives too! We are not one-size-fits-all, so a midwife that was right for your family member or friend, may not meet your individual needs or jive with your philosophy. Please carefully interview your potential provider with hard questions! Transparency is *key* to trusting your birth attendant!)
If your provider says any variation of the following:
“We might be able to support that”, “We don’t allow that”, “Hospital policy says…”, “I can’t let you…”
“I calculated your VBAC success rate & it’s looking low, you probably won’t be able to achieve a VBAC…”
“You should get an epidural, just in case”
“You’ll need to have continuous fetal monitoring or internal fetal monitoring, just in case”
“Let’s schedule a cesarean, it’s better for both of our schedules”
“Your babies are too close together”
“You haven’t dilated yet, so you probably won’t go into labor by 40/41 weeks”
“Your baby is just too big to fit” (prior to TOLAC)
“Once a cesarean, always a cesarean”
Or you experience any of the following:
Leaving appointments feeling unsupported / Feeling like you may need to “fight” for the birth you desire or feeling like you may need to “give in” to your provider
Restrictions on pregnancy duration, restrictions on labor duration or restrictions on time “allowed” for pushing
Care that is *not* based on current research/evidence
Remember to ask hard questions like
“What is your primary cesarean rate” or “What is your VBAC success rate?”
“What are your beliefs regarding big babies or macrosomia?”
“Do you place restrictions on pregnancy/labor/pushing duration?”
Remember that it’s never too late to transfer providers. I had the pleasure of caring for a young woman while I was finishing my training, who transferred to our care at 38 weeks. She was having her second baby, 1st was around 9lbs and delivered vaginally. Her second baby was projected to be “large” and her provider was strongly pushing a cesarean on her. She firmly believed in her body’s ability to birth and decided to find a more supportive provider. She rocked a water birth at the birth center for her baby who weighed 10lbs 2oz!! (Though I think those 2 extra ounces was her hair alone!) And although she was not a VBAC, this is a great example of how women *do* get suckered into having an unnecessary cesarean delivery.



Fun Facts!
Barefoot Birth VBAC & cesarean stats (as a whole for the practice in 2015)
VBAC: 66% success rate (including high order & special scar clients), 10% cesarean rate (2% primary, 8% secondary), 8% of all births in 2015 were VBACs!
29 moms who reside in Hernando County delivered in Out-of-Hospital settings! This includes moms who travelled to a free-standing birth center. 16 of those moms had a home birth with a licensed midwife and 1 delivered unassisted or with an unknown birth attendant.
I was one of those 16 home births with a licensed midwife!
Recommended reads for women who have had a cesarean and want to know more about VBAC:
Thinking Woman’s Guide to a Better Birth by Henci Goer
Second Chance: A Mother's Quest for a Natural Birth after a Cesarean by Thais Nye Derich
Silent Knife: Cesarean Prevention & VBAC by Lois J Estner
Birthing Normally After a Cesarean or Two by H. L. Ne Vadeboncoeur
Vaginal Birth After Caesarean: The VBAC Handbook by Helen Churchill
So, what are your VBAC options in Spring Hill, FL??
Many hospital-based providers advertise that they are currently offering trial-of-labor-after-cesarean or TOLAC. Meaning they will let you go into labor naturally (usually with hidden criteria) and if you “happen” to deliver vaginally, then you will have successfully had a VBAC. Most of the time, the criteria is very strict and many providers pull some of the preceding VBAC sabotages just a few weeks before you deliver. At that point you are invested in & trust that provider and/or too afraid to get a second opinion. And just like that, you get duped into an unnecessary cesarean delivery. Well now families in Hernando County and surrounding areas have the option for a safe, supportive & alternative birth experience. Where VBAC is not only encouraged, but very attainable. Barefoot Birth is one of the only providers that will consider “special scar” incisions and previous cesareans of high-order. Let’s work towards not only increasing the number of home births here, but on improving all of these birth statistics and increasing the chances of achieving VBAC!
Contact Erica, Licensed Midwife serving an hour radius of Hernando County, for a free consultation! 352.584.5113 I'd love to meet with you to discuss your options!
Credit to ImprovingBirth.org, BellyBelly.com.au and Scattered Seashells for their VBAC sabotages & myths lists
Also, feel free to check out the World Health Organization’s C-Model, to determine what your probability is for a cesarean or likelihood of a VBAC, before your provider can use it against you...
Love and Light, Barefoot Family! ~Erica